
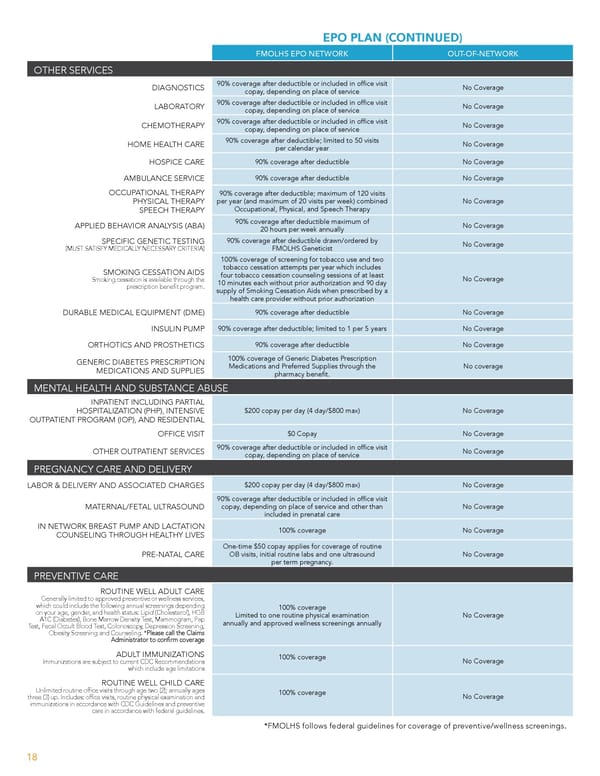
EPO PLAN (CONTINUED) FMOLHS EPO NETWORK OUT-OF-NETWORK OTHER SERVICES 90% coverage after deductible or included in of昀椀ce visit DIAGNOSTICS No Coverage copay, depending on place of service 90% coverage after deductible or included in of昀椀ce visit LABORATORY No Coverage copay, depending on place of service 90% coverage after deductible or included in of昀椀ce visit CHEMOTHERAPY No Coverage copay, depending on place of service 90% coverage after deductible; limited to 50 visits HOME HEALTH CARE No Coverage per calendar year HOSPICE CARE 90% coverage after deductible No Coverage AMBULANCE SERVICE 90% coverage after deductible No Coverage OCCUPATIONAL THERAPY 90% coverage after deductible; maximum of 120 visits PHYSICAL THERAPY per year (and maximum of 20 visits per week) combined No Coverage SPEECH THERAPY Occupational, Physical, and Speech Therapy 90% coverage after deductible maximum of APPLIED BEHAVIOR ANALYSIS (ABA) No Coverage 20 hours per week annually SPECIFIC GENETIC TESTING 90% coverage after deductible drawn/ordered by (MUST SATISFY MEDICALLY NECESSARY CRITERIA) FMOLHS Geneticist No Coverage 100% coverage of screening for tobacco use and two SMOKING CESSATION AIDS tobacco cessation attempts per year which includes four tobacco cessation counseling sessions of at least Smoking cessation is available through the No Coverage 10 minutes each without prior authorization and 90 day prescription bene昀椀t program. supply of Smoking Cessation Aids when prescribed by a health care provider without prior authorization DURABLE MEDICAL EQUIPMENT (DME) 90% coverage after deductible No Coverage INSULIN PUMP 90% coverage after deductible; limited to 1 per 5 years No Coverage ORTHOTICS AND PROSTHETICS 90% coverage after deductible No Coverage GENERIC DIABETES PRESCRIPTION 100% coverage of Generic Diabetes Prescription MEDICATIONS AND SUPPLIES Medications and Preferred Supplies through the No coverage pharmacy bene昀椀t. MENTAL HEALTH AND SUBSTANCE ABUSE INPATIENT INCLUDING PARTIAL HOSPITALIZATION (PHP), INTENSIVE $200 copay per day (4 day/$800 max) No Coverage OUTPATIENT PROGRAM (IOP), AND RESIDENTIAL OFFICE VISIT $0 Copay No Coverage 90% coverage after deductible or included in of昀椀ce visit OTHER OUTPATIENT SERVICES No Coverage copay, depending on place of service PREGNANCY CARE AND DELIVERY LABOR & DELIVERY AND ASSOCIATED CHARGES $200 copay per day (4 day/$800 max) No Coverage 90% coverage after deductible or included in of昀椀ce visit MATERNAL/FETAL ULTRASOUND copay, depending on place of service and other than No Coverage included in prenatal care IN NETWORK BREAST PUMP AND LACTATION COUNSELING THROUGH HEALTHY LIVES 100% coverage No Coverage One-time $50 copay applies for coverage of routine PRE-NATAL CARE OB visits, initial routine labs and one ultrasound No Coverage per term pregnancy. PREVENTIVE CARE ROUTINE WELL ADULT CARE Generally limited to approved preventive or wellness services, which could include the following annual screenings depending 100% coverage on your age, gender, and health status: Lipid (Cholesterol), HGB Limited to one routine physical examination No Coverage A1C (Diabetes), Bone Marrow Density Test, Mammogram, Pap annually and approved wellness screenings annually Test, Fecal Occult Blood Test, Colonoscopy, Depression Screening, Obesity Screening and Counseling. *Please call the Claims Administrator to con昀椀rm coverage ADULT IMMUNIZATIONS 100% coverage No Coverage Immunizations are subject to current CDC Recommendations which include age limitations ROUTINE WELL CHILD CARE Unlimited routine of昀椀ce visits through age two (2); annually ages 100% coverage No Coverage three (3) up. Includes: of昀椀ce visits, routine physical examination and immunizations in accordance with CDC Guidelines and preventive care in accordance with federal guidelines. *FMOLHS follows federal guidelines for coverage of preventive/wellness screenings. 18
 Team Member Guide to Benefit Enrollment Page 17 Page 19
Team Member Guide to Benefit Enrollment Page 17 Page 19