
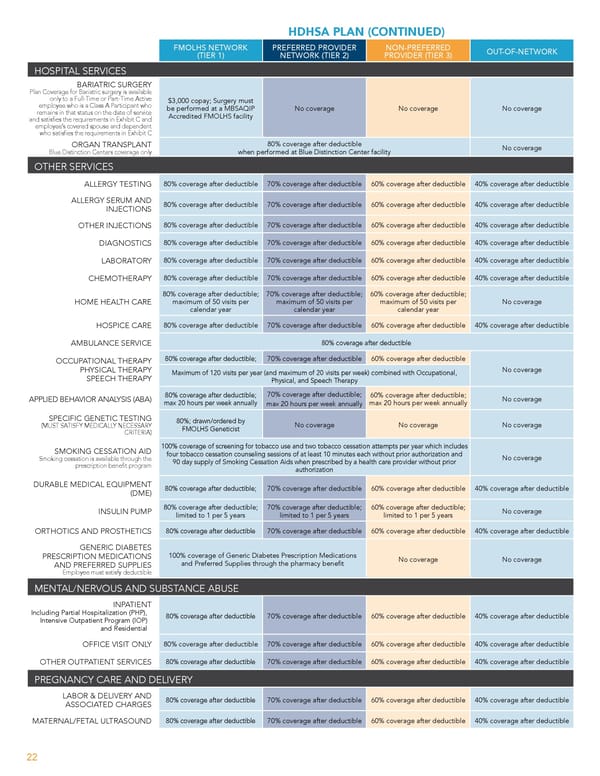
HDHSA PLAN (CONTINUED) FMOLHS NETWORK PREFERRED PROVIDER NON-PREFERRED OUT-OF-NETWORK (TIER 1) NETWORK (TIER 2) PROVIDER (TIER 3) HOSPITAL SERVICES BARIATRIC SURGERY Plan Coverage for Bariatric surgery is available only to a Full-Time or Part-Time Active $3,000 copay; Surgery must employee who is a Class A Participant who be performed at a MBSAQIP No coverage No coverage No coverage remains in that status on the date of service Accredited FMOLHS facility and satis昀椀es the requirements in Exhibit C and employee’s covered spouse and dependent who satis昀椀es the requirements in Exhibit C ORGAN TRANSPLANT 80% coverage after deductible No coverage Blue Distinction Centers coverage only when performed at Blue Distinction Center facility OTHER SERVICES ALLERGY TESTING 80% coverage after deductible 70% coverage after deductible 60% coverage after deductible 40% coverage after deductible ALLERGY SERUM AND INJECTIONS 80% coverage after deductible 70% coverage after deductible 60% coverage after deductible 40% coverage after deductible OTHER INJECTIONS 80% coverage after deductible 70% coverage after deductible 60% coverage after deductible 40% coverage after deductible DIAGNOSTICS 80% coverage after deductible 70% coverage after deductible 60% coverage after deductible 40% coverage after deductible LABORATORY 80% coverage after deductible 70% coverage after deductible 60% coverage after deductible 40% coverage after deductible CHEMOTHERAPY 80% coverage after deductible 70% coverage after deductible 60% coverage after deductible 40% coverage after deductible 80% coverage after deductible; 70% coverage after deductible; 60% coverage after deductible; HOME HEALTH CARE maximum of 50 visits per maximum of 50 visits per maximum of 50 visits per No coverage calendar year calendar year calendar year HOSPICE CARE 80% coverage after deductible 70% coverage after deductible 60% coverage after deductible 40% coverage after deductible AMBULANCE SERVICE 80% coverage after deductible OCCUPATIONAL THERAPY 80% coverage after deductible; 70% coverage after deductible 60% coverage after deductible PHYSICAL THERAPY No coverage SPEECH THERAPY Maximum of 120 visits per year (and maximum of 20 visits per week) combined with Occupational, Physical, and Speech Therapy 70% coverage after deductible; 80% coverage after deductible; 60% coverage after deductible; APPLIED BEHAVIOR ANALYSIS (ABA) No coverage max 20 hours per week annually max 20 hours per week annually max 20 hours per week annually SPECIFIC GENETIC TESTING 80%; drawn/ordered by (MUST SATISFY MEDICALLY NECESSARY No coverage No coverage No coverage CRITERIA) FMOLHS Geneticist SMOKING CESSATION AID 100% coverage of screening for tobacco use and two tobacco cessation attempts per year which includes four tobacco cessation counseling sessions of at least 10 minutes each without prior authorization and No coverage Smoking cessation is available through the 90 day supply of Smoking Cessation Aids when prescribed by a health care provider without prior prescription bene昀椀t program authorization DURABLE MEDICAL EQUIPMENT (DME) 80% coverage after deductible; 70% coverage after deductible 60% coverage after deductible 40% coverage after deductible 80% coverage after deductible; 70% coverage after deductible; 60% coverage after deductible; INSULIN PUMP No coverage limited to 1 per 5 years limited to 1 per 5 years limited to 1 per 5 years ORTHOTICS AND PROSTHETICS 80% coverage after deductible 70% coverage after deductible 60% coverage after deductible 40% coverage after deductible GENERIC DIABETES PRESCRIPTION MEDICATIONS 100% coverage of Generic Diabetes Prescription Medications No coverage No coverage AND PREFERRED SUPPLIES and Preferred Supplies through the pharmacy bene昀椀t Employee must satisfy deductible MENTAL/NERVOUS AND SUBSTANCE ABUSE INPATIENT Including Partial Hospitalization (PHP), 80% coverage after deductible 70% coverage after deductible 60% coverage after deductible 40% coverage after deductible Intensive Outpatient Program (IOP) and Residential OFFICE VISIT ONLY 80% coverage after deductible 70% coverage after deductible 60% coverage after deductible 40% coverage after deductible OTHER OUTPATIENT SERVICES 80% coverage after deductible 70% coverage after deductible 60% coverage after deductible 40% coverage after deductible PREGNANCY CARE AND DELIVERY LABOR & DELIVERY AND ASSOCIATED CHARGES 80% coverage after deductible 70% coverage after deductible 60% coverage after deductible 40% coverage after deductible MATERNAL/FETAL ULTRASOUND 80% coverage after deductible 70% coverage after deductible 60% coverage after deductible 40% coverage after deductible 22
 Team Member Guide to Benefit Enrollment Page 21 Page 23
Team Member Guide to Benefit Enrollment Page 21 Page 23