
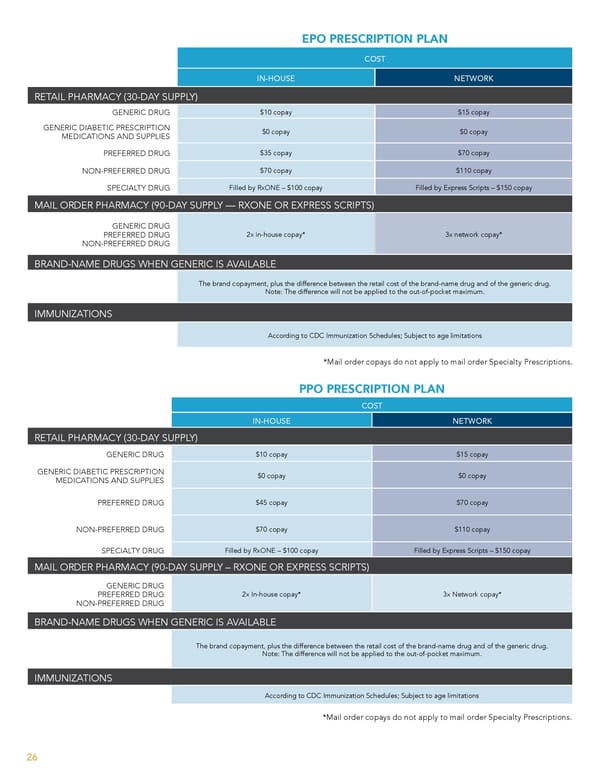
EPO PRESCRIPTION PLAN COST IN-HOUSE NETWORK RETAIL PHARMACY (30-DAY SUPPLY) GENERIC DRUG $10 copay $15 copay GENERIC DIABETIC PRESCRIPTION MEDICATIONS AND SUPPLIES $0 copay $0 copay PREFERRED DRUG $35 copay $70 copay NON-PREFERRED DRUG $70 copay $110 copay SPECIALTY DRUG Filled by RxONE – $100 copay Filled by Express Scripts – $150 copay MAIL ORDER PHARMACY (90-DAY SUPPLY — RXONE OR EXPRESS SCRIPTS) GENERIC DRUG PREFERRED DRUG 2x in-house copay* 3x network copay* NON-PREFERRED DRUG BRAND-NAME DRUGS WHEN GENERIC IS AVAILABLE The brand copayment, plus the difference between the retail cost of the brand-name drug and of the generic drug. Note: The difference will not be applied to the out-of-pocket maximum. IMMUNIZATIONS According to CDC Immunization Schedules; Subject to age limitations *Mail order copays do not apply to mail order Specialty Prescriptions. PPO PRESCRIPTION PLAN COST IN-HOUSE NETWORK RETAIL PHARMACY (30-DAY SUPPLY) GENERIC DRUG $10 copay $15 copay GENERIC DIABETIC PRESCRIPTION MEDICATIONS AND SUPPLIES $0 copay $0 copay PREFERRED DRUG $45 copay $70 copay NON-PREFERRED DRUG $70 copay $110 copay SPECIALTY DRUG Filled by RxONE – $100 copay Filled by Express Scripts – $150 copay MAIL ORDER PHARMACY (90-DAY SUPPLY – RXONE OR EXPRESS SCRIPTS) GENERIC DRUG PREFERRED DRUG 2x In-house copay* 3x Network copay* NON-PREFERRED DRUG BRAND-NAME DRUGS WHEN GENERIC IS AVAILABLE The brand copayment, plus the difference between the retail cost of the brand-name drug and of the generic drug. Note: The difference will not be applied to the out-of-pocket maximum. IMMUNIZATIONS According to CDC Immunization Schedules; Subject to age limitations *Mail order copays do not apply to mail order Specialty Prescriptions. 26
 Team Member Guide to Benefit Enrollment Page 25 Page 27
Team Member Guide to Benefit Enrollment Page 25 Page 27