
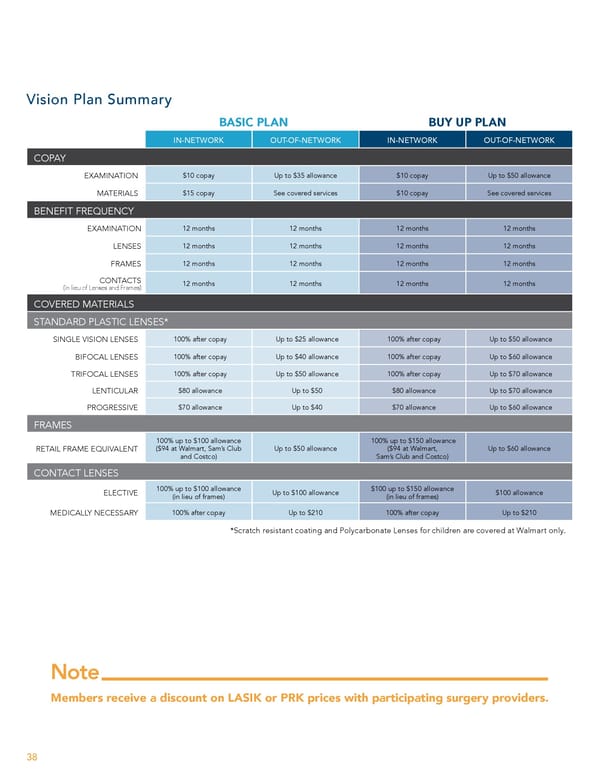
Vision Plan Summary BASIC PLAN BUY UP PLAN IN-NETWORK OUT-OF-NETWORK IN-NETWORK OUT-OF-NETWORK COPAY EXAMINATION $10 copay Up to $35 allowance $10 copay Up to $50 allowance MATERIALS $15 copay See covered services $10 copay See covered services BENEFIT FREQUENCY EXAMINATION 12 months 12 months 12 months 12 months LENSES 12 months 12 months 12 months 12 months FRAMES 12 months 12 months 12 months 12 months CONTACTS 12 months 12 months 12 months 12 months (in lieu of Lenses and Frames) COVERED MATERIALS STANDARD PLASTIC LENSES* SINGLE VISION LENSES 100% after copay Up to $25 allowance 100% after copay Up to $50 allowance BIFOCAL LENSES 100% after copay Up to $40 allowance 100% after copay Up to $60 allowance TRIFOCAL LENSES 100% after copay Up to $50 allowance 100% after copay Up to $70 allowance LENTICULAR $80 allowance Up to $50 $80 allowance Up to $70 allowance PROGRESSIVE $70 allowance Up to $40 $70 allowance Up to $60 allowance FRAMES 100% up to $100 allowance 100% up to $150 allowance RETAIL FRAME EQUIVALENT ($94 at Walmart, Sam’s Club Up to $50 allowance ($94 at Walmart, Up to $60 allowance and Costco) Sam’s Club and Costco) CONTACT LENSES 100% up to $100 allowance $100 up to $150 allowance ELECTIVE Up to $100 allowance $100 allowance (in lieu of frames) (in lieu of frames) MEDICALLY NECESSARY 100% after copay Up to $210 100% after copay Up to $210 *Scratch resistant coating and Polycarbonate Lenses for children are covered at Walmart only. Note Members receive a discount on LASIK or PRK prices with participating surgery providers. 38
 Team Member Guide to Benefit Enrollment Page 37 Page 39
Team Member Guide to Benefit Enrollment Page 37 Page 39