
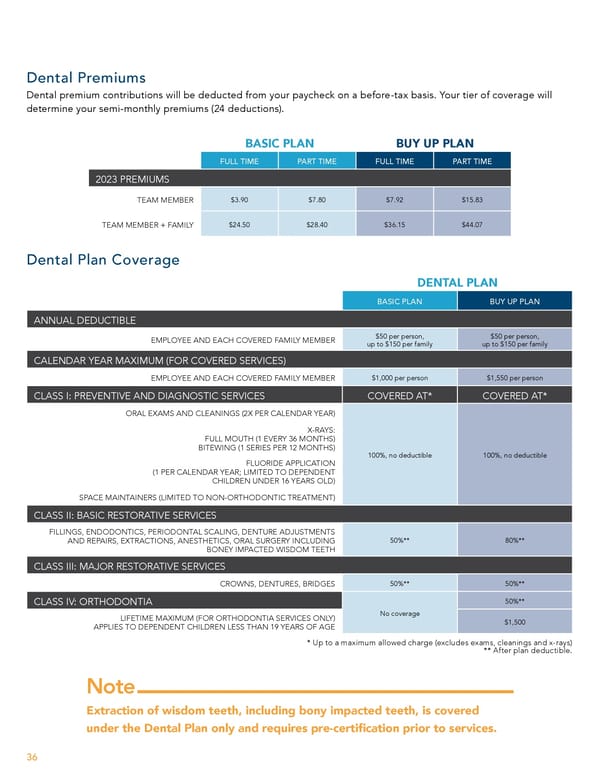
Dental Premiums Dental premium contributions will be deducted from your paycheck on a before-tax basis. Your tier of coverage will determine your semi-monthly premiums (24 deductions). BASIC PLAN BUY UP PLAN FULL TIME PART TIME FULL TIME PART TIME 2023 PREMIUMS TEAM MEMBER $3.90 $7.80 $7.92 $15.83 TEAM MEMBER + FAMILY $24.50 $28.40 $36.15 $44.07 Dental Plan Coverage DENTAL PLAN BASIC PLAN BUY UP PLAN ANNUAL DEDUCTIBLE EMPLOYEE AND EACH COVERED FAMILY MEMBER $50 per person, $50 per person, up to $150 per family up to $150 per family CALENDAR YEAR MAXIMUM (FOR COVERED SERVICES) EMPLOYEE AND EACH COVERED FAMILY MEMBER $1,000 per person $1,550 per person CLASS I: PREVENTIVE AND DIAGNOSTIC SERVICES COVERED AT* COVERED AT* ORAL EXAMS AND CLEANINGS (2X PER CALENDAR YEAR) X-RAYS: FULL MOUTH (1 EVERY 36 MONTHS) BITEWING (1 SERIES PER 12 MONTHS) 100%, no deductible 100%, no deductible FLUORIDE APPLICATION (1 PER CALENDAR YEAR; LIMITED TO DEPENDENT CHILDREN UNDER 16 YEARS OLD) SPACE MAINTAINERS (LIMITED TO NON-ORTHODONTIC TREATMENT) CLASS II: BASIC RESTORATIVE SERVICES FILLINGS, ENDODONTICS, PERIODONTAL SCALING, DENTURE ADJUSTMENTS AND REPAIRS, EXTRACTIONS, ANESTHETICS, ORAL SURGERY INCLUDING 50%** 80%** BONEY IMPACTED WISDOM TEETH CLASS III: MAJOR RESTORATIVE SERVICES CROWNS, DENTURES, BRIDGES 50%** 50%** 50%** CLASS IV: ORTHODONTIA LIFETIME MAXIMUM (FOR ORTHODONTIA SERVICES ONLY) No coverage APPLIES TO DEPENDENT CHILDREN LESS THAN 19 YEARS OF AGE $1,500 * Up to a maximum allowed charge (excludes exams, cleanings and x-rays) ** After plan deductible. Note Extraction of wisdom teeth, including bony impacted teeth, is covered under the Dental Plan only and requires pre-certi昀椀cation prior to services. 36
 Team Member Guide to Benefit Enrollment Page 35 Page 37
Team Member Guide to Benefit Enrollment Page 35 Page 37